
Scales. Decades of cerebral palsy research suddenly become meaningful for STXBP1 and SYNGAP1. The CP field has built a mature framework of classification systems such as the Gross Motor Function Classification System (GMFCS), along with related tools for manual ability and communication. These systems were not developed for synaptic disorders, which were largely unknown when these scales were first conceptualized. However, as we move toward trial readiness, they offer exactly what we need: structured ways to describe function. The question is whether they translate and can be used. Here is what we found.
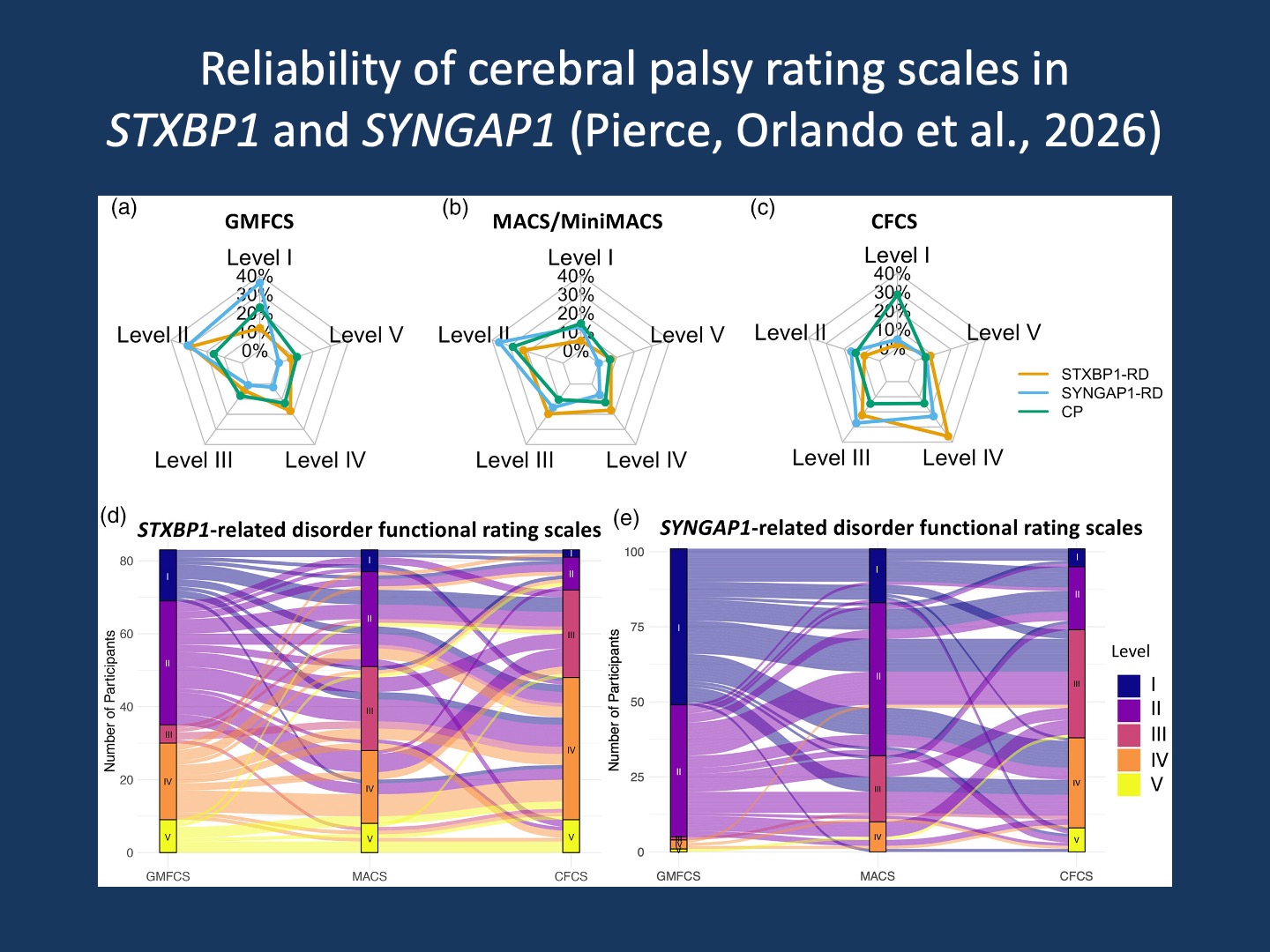
Figure. This figure shows how individuals with STXBP1-related and SYNGAP1-related disorders distribute across commonly used cerebral palsy classification systems and how these classifications relate to each other. Panels (a–c) display the proportion of individuals in each severity level (Levels I–V) for gross motor function (GMFCS), manual ability (MACS/Mini-MACS), and communication (CFCS), compared to a reference cerebral palsy (CP) cohort. These levels range from more independent function (Level I) to more significant support needs (Level V), providing a structured way to describe ability across domains.
Panels (d,e) take this one step further by connecting each individual’s classification across the three systems. Each line represents one person, linking their motor, manual, and communication levels. Rather than collapsing function into a single score, this visualization shows how individuals occupy different positions across domains. What becomes visible is that these conditions are not one-dimensional: a given level of motor function does not necessarily predict communication or manual ability. This multidimensional pattern is exactly what these classification systems allow us to capture (Figure 1 from Pierce, Orlando et al., 2026).
Our approach. In our study by Pierce, Orlando et al., we examined whether cerebral palsy-derived classification systems behave reliably and consistently in STXBP1-related and SYNGAP1-related disorders. Reliability and consistency of these scales is more important than it might look like at first glance. While these scales are already used widely in neurogenetics, we are making quite a few assumptions about whether they are actually appropriate. The disease mechanism in CP is different from synapse disorders. And with the dynamic and sometimes unexpected changes we often see in patient trajectories, demonstrating that these scales are reliable is a critical piece of the trial readiness puzzle.
Two scale types. It is useful to distinguish the classification systems we examined in our study by Pierce and collaborators from quantitative developmental measures such as the Gross Motor Function Measure (GMFM), the Bayley Scales of Infant and Toddler Development, or the Peabody Developmental Motor Scales. Classification systems group individuals into levels based on function, providing a shared clinical language. Quantitative scales, in contrast, assign numerical scores intended to track change over time. Both are essential, but they answer different questions. Classification systems help us understand where an individual is within a functional landscape, while quantitative measures attempt to capture movement within that landscape. Here are the classification scales that we looked at.
GMFCS. The Gross Motor Function Classification System captures mobility, from independent walking to limited self-mobility. In our cohort, interrater reliability for GMFCS was strong, with consistent agreement across clinicians. This is a key finding. It shows that even in synaptic disorders, we can describe motor function in a structured and reproducible way. However, some individuals changed GMFCS levels over time, which points to the dynamic nature of development in synaptic disorders.
MACS. The Manual Ability Classification System focuses on hand use in daily activities. Here, we saw the same pattern of strong agreement across raters, reinforcing that manual ability can be captured consistently in STXBP1 and SYNGAP1. At the same time, the presence of change over time highlights that these classifications are not static labels and that hand function can evolve in synaptic disorders.
CFCS. The Communication Function Classification System extends this framework to communication. Reliability on the CFCS remained solid, supporting its use in this domain in STXBP1 and SYNGAP1. Variability over time was again observed, particularly in SYNGAP1, pointing to the complexity of communication trajectories in neurodevelopmental disorders, especially those with a strong autism and behavioral contribution.
What works. Taken together, our findings show that these classification systems do more than just work, they actually provide a pretty good (i.e. robust and reproducible) framework for describing function in STXBP1 and SYNGAP1. This now creates a common language that can be used across studies, sites, and clinical contexts. For a field moving toward clinical trials, this is an important foundational step, and it also unlocks decades of CP research for us, where classification systems such as GMFCS became more than just descriptive tools. In the CP field, these classification systems enabled the construction of developmental trajectories and informed expectations about change. Our findings suggest that a similar trajectory is possible for STXBP1 and SYNGAP1.
Trial readiness. For natural history studies such as STARR (STXBP1) and ProMMiS (SYNGAP1), this is highly relevant. Regulatory decisions depend on outcome measures that have been shown to be reliable and interpretable. Our study shows that these tools provide a strong starting point. At the same time, the observed variability over time highlights the need to understand how changes in classification relate to clinically meaningful outcomes. This will be the next phase of our work in moving these conditions towards trial readiness.
What you need to know. In our study by Pierce, Orlando et al., we show that cerebral palsy classification systems such as GMFCS, MACS, and CFCS perform well in STXBP1 and SYNGAP1, with strong interrater reliability and meaningful sensitivity to developmental change. These tools provide a practical and scalable framework for outcome assessment and trial readiness in studies such as STARR and ProMMiS. At the same time, their behavior points to the next set of questions: how to interpret change over time and how to translate these changes into clinically meaningful endpoints in synaptic disorders.